
How do antidepressants work?

To understand how antidepressants work, you need to understand some basic neuroscience of depression.
There are two sets of theories that explain how antidepressants work.
1) Neurochemical theories
The first set of theories is neurochemical theories. These theories propose that antidepressant medications work by regulating different neurotransmitter and their receptors. The basic idea is that the root of depression symptoms lies in a lack, or an imbalance, of certain brain chemicals.
First, we need to understand how antidepressants alter our neurochemical levels fully. (Each group of antidepressants has a different mechanism of action, so I will use SSRIs as an example.)
Our brain is made up of a complex and interconnected web of cells. These cells are called neurons (or nerve cells) and make up the basis of our nervous system. From the day these cells are developed to the last day of our lives, these cells constantly communicate with each other. A group of two neurons that communicate with each other is called a synapse. Two neurons that make a synapse are divided by a huge gap (on the scale of neurons) called the synaptic gap.
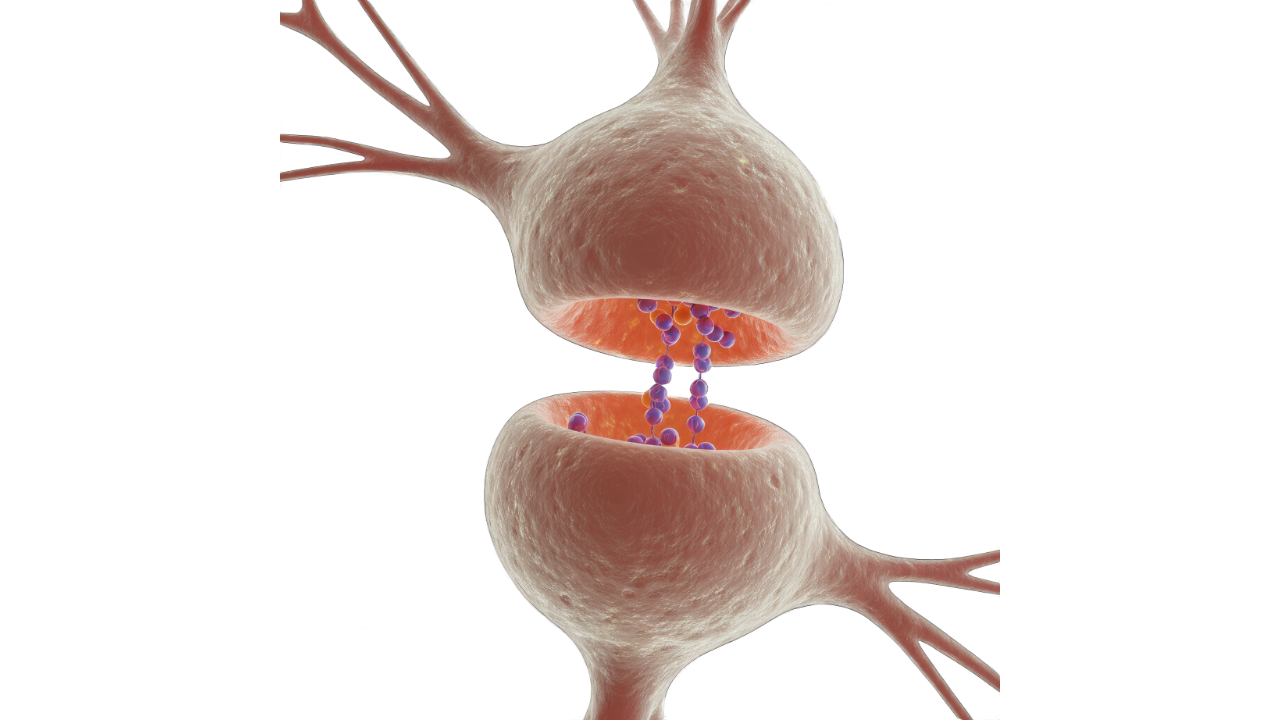
To traverse that gap and “talk” effectively, neurons release a chemical signal or molecules called neurotransmitters. You probably heard about neurotransmitters, and some of the most popular are serotonin, norepinephrine, dopamine, glutamate, and GABA. A group of neurons that release a specific neurotransmitter is given names based on the neurotransmitter they release.
For example, neurons that use serotonin to communicate are called serotonergic neurons, and the ones that use dopamine are called dopaminergic neurons. So a neurotransmitter (serotonin in this case) is released from one end of a neuron into the synaptic gap and binds to its receptor on the end of another neuron. By binding to its receptor, serotonin activates a multitude of molecular changes inside the other neuron, thus transferring the signal from the original neuron.
Once the signal has been transferred, serotonin is released from its receptor and pulled out of (reuptake) a synaptic gap either by the original neuron or another type of nerve cell called a glial cell.
Bear with me for now.
The mechanism by which serotonin leaves the gap and enters its original neuron is incredibly simple. Once serotonin finds itself in the synaptic gap, it binds to another receptor on the original neuron called the Serotonin transporter (SERT). The serotonin transporter then reuptakes the serotonin left in the gap and stores it in the original neuron for later repurposing.
You should by now ask yourself why the neuron takes the neurotransmitter it already released. The answer is really simple. This reuptake process is a real example of how our body minimizes energy expenditure by repurposing every material it can. Would you buy a new fridge if the old one still functions properly? No? Then why would the brain want to synthesize a new neurotransmitter if the old one still works properly?
Now that you understand how neurons communicate, you can also understand how SSRIs affect the reuptake of serotonin.
SSRIs work by inhibiting the Serotonin transporter (SERT) consequentially inhibiting the reuptake of serotonin to its original neuron. This way, much more serotonin is left in the synaptic gap, ready to once again bind to its receptors and allow the neuron communication to happen.
At first, researchers thought that this simple rise in certain neurotransmitter concentrations proved enough to reduce depression symptoms. However, it was observed that SSRI antidepressants almost immediately increase the amount of serotonin in the brain, but they take a few weeks to start reducing your depression symptoms. So where does that delay of action come from?
The newer idea that supports neurochemical theories is that of the 5-HT1a receptor. The name 5-HT comes from 5-hydroxytryptamine and is just another name for serotonin based on its chemical structure. The 5-HT1a receptor is a serotonin receptor that inhibits the action of serotonergic neurons (the ones that release serotonin) once a molecule of serotonin is bound to it.
It serves as a neuromodulator, preventing the too frequent firing of serotonergic neurons.
Once we take SSRIs and inhibit our SERT transporter, more and more serotonin is accumulated in the synapse. At first, the 5-HT1a receptor does its aforementioned job in preventing the frequent firing of a serotonergic neuron, but there’s a catch. As more and more serotonin binds to the 5-HT1a receptor, the serotonergic neuron actively starts reducing the number of 5-HT1a receptors.
This process is called receptor downregulation and is useful in a variety of physiological events. By lowering the number of certain receptors, our cells balance how much of an effect a certain molecule will have.
Take insulin, for example. If, for whatever reason, our blood insulin concentration rises dramatically, we would fall into severe hypoglycemia and suffer its devastating effects. However, by reducing the number of insulin receptors, our cells provide a safety mechanism and prevent such occurrences since the effects of insulin (no matter how high its blood concentration is) are now limited by the number of its receptors.
The same goes for the 5-HT1a receptor:
Once downregulation does its job, the nerve cells are left with a much lower number of 5-HT1a receptors that cannot inhibit the frequent serotonergic firing, no matter how high the blood serotonin concentration is.
This theory makes much more sense because downregulation is mediated by all sorts of molecular mechanisms and takes a few weeks to occur. This delayed time of action perfectly fits the time it takes to see the first alleviation in depressive symptoms of individuals starting an antidepressant regimen.
2) Neuroplasticity theories
The second sets of theories include neuroplasticity theories.
Brain plasticity or neuroplasticity is an umbrella term that refers to the brain’s ability to modify, change, and adapt both its structure and function throughout life and in response to different experiences.
People usually make the mistake of thinking that the brain is some form of distant entity, not affected by the rest of their body. When talking about the brain, you can easily fall into the trap of believing that the brain is somehow detached from the rest of your organ systems, or everyday events, for that matter.
It is important to understand that the brain is, just like your heart, for example, a living organ and is under the effects of various physiological and psychological events. The brain is “plastic,” ie, it can change in response to stress, anxiety, trauma, and depression.

When talking about neuroplasticity theories in the context of depression, it is necessary to mention a few different aspects of depression-related brain changes. The first aspect is the effect of stress on our brain circuits, primarily circuits in our prefrontal cortex and limbic system that govern our cognition, memory, and emotions.
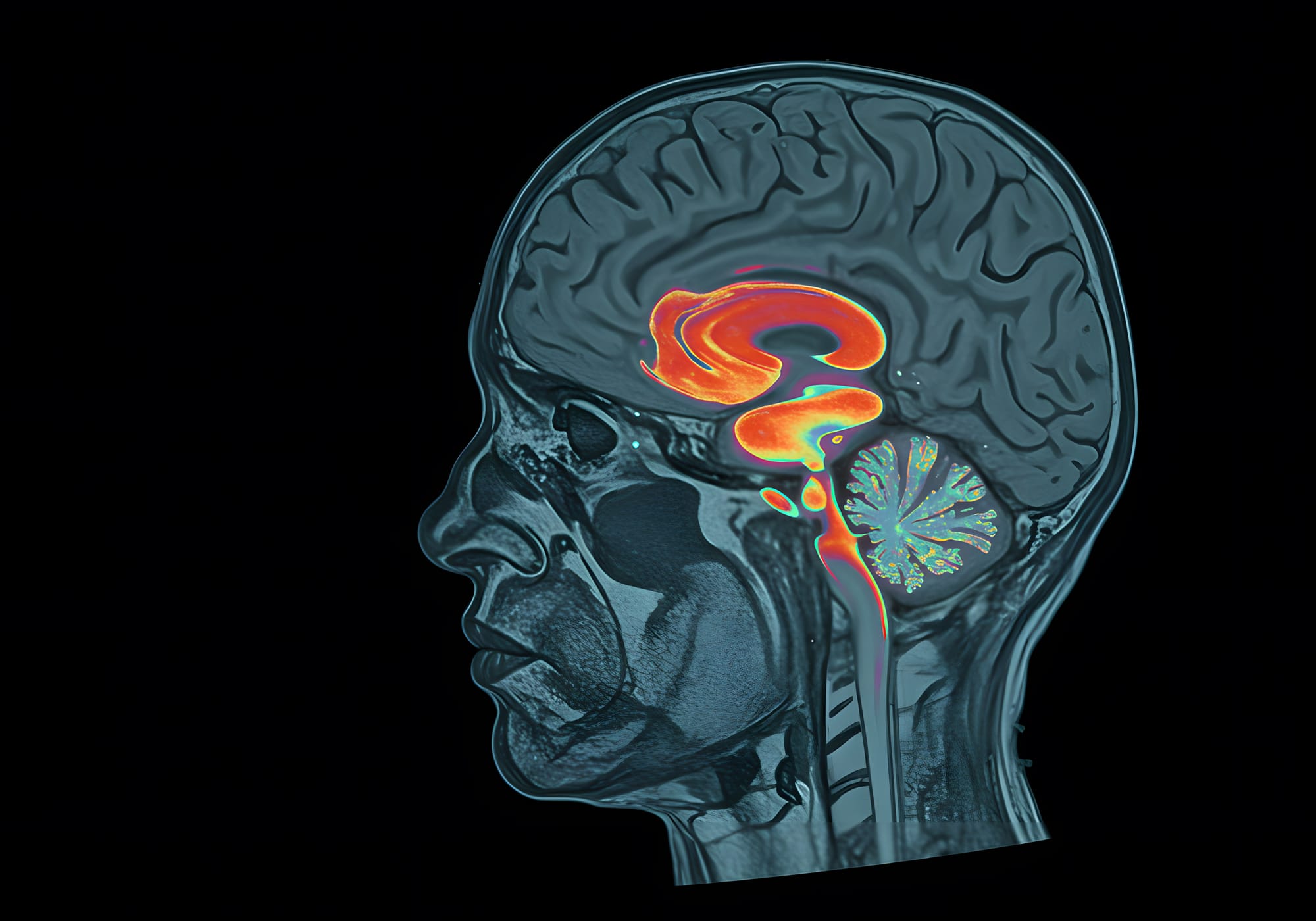
Long-term stress is capable of reducing the number of dendritic spines and synapses, inducing loss of glia, and even impairing neurogenesis (formation of new neurons). With that said, it is truly fascinating that with modern imaging technology, we can see the physical changes in brain architecture. Those changes are particularly seen in people suffering from anxiety and/or depression.
Research showed a significant reduction in hippocampal volume in post-mortem (after-death) animals subjected to various stressors and an equal reduction of hippocampal volume in MRIs of depressed human individuals. Since the hippocampus is one of the main brain structures responsible for learning and forming new memories, it is logical to assume that people suffering from depression might struggle with these cognitive tasks.
The evidence for such “shrinkage” is not constrained to the hippocampus only but is evident in many parts of the brain.
The prefrontal cortex, for example, is a part of the brain in charge of our higher cognitive functions like concentration, attention, language, abstraction, and planning. From different neuroimaging techniques, we can see that the depression-affected brain shows lessened activity in the prefrontal cortex.
"In other words, when people are depressed, they find it profoundly difficult to set certain goals for themselves, but also lack proper concentration and motivation to achieve those goals."
Another function of the prefrontal cortex that is reduced in depressed individuals is its ability to inhibit negative emotions generated by limbic structures such as the amygdala.
In contrast to changes caused by anxiety and depression, research showed that antidepressants are associated with the induction of neuroplasticity in different brain structures, such as the hippocampus and prefrontal cortex. The neuroplasticity that occurs in these regions of the brain is due to stimulation of neurogenesis, new synapse formation, and the arborization of dendritic spines.
So, in people suffering from depression, we can clearly see that the brain literally changes its structure, and those changes are reversible through an antidepressant regimen. One more important piece of information to notice is that it takes a few weeks for the brain’s structural changes to occur. This notion parallels the one from the neurochemical theory of depression, and the time delay with neuroplasticity fits almost perfectly with the time it takes antidepressants to start working.
In conclusion, the two theories are equally valid and can explain the mechanism of the antidepressant best if used in combination. By increasing the concentration of certain neurotransmitters, antidepressant drugs induce brain plasticity and reverse some of the damage caused by anxiety and/or depression.
In summary:
1. Neurochemical Theories
- Depression is partly caused by imbalances in brain chemicals, especially neurotransmitters like serotonin.
- SSRIs (Selective Serotonin Reuptake Inhibitors) increase serotonin levels by blocking its reuptake via the SERT transporter, leaving more serotonin in the synapse to stimulate communication between neurons.
- However, antidepressants don't work instantly. This delay is explained by 5-HT1a receptor downregulation:
- Initially, increased serotonin activates 5-HT1a receptors, which inhibit further serotonin release.
- Over time, the brain reduces the number of these receptors (downregulation), allowing serotonin neurons to fire more freely, which correlates with symptom improvement after a few weeks.
2. Neuroplasticity Theories
- Depression also involves physical changes in the brain, especially due to chronic stress, which can shrink areas like the hippocampus and prefrontal cortex.
- These areas are important for memory, emotion regulation, and decision-making.
- Antidepressants help reverse these changes by:
- Stimulating neurogenesis (new neurons),
- Promoting new synapse formation, and
- Enhancing dendritic growth (connections between neurons).
- Like the neurochemical effects, these structural changes take several weeks, which matches the delayed symptom relief.
Conclusion
Antidepressants likely work through a combination of both mechanisms:
- Short-term: Increasing neurotransmitter levels (especially serotonin).
- Long-term: Promoting brain repair and adaptability through neuroplasticity.
These combined effects help improve mood, cognition, and emotional regulation in people with depression.