
Ketamine and Depression


The diagnosis and treatment of depression remain one of the most elusive tasks of today’s medicine. While there has been a somewhat successful treatment of depressive disorders using SSRIs and SNRIs, I stumbled upon devastating and concerning statistics.
Nearly one-third of all patients with depression fail to respond to standard treatment.
The cause for this phenomenon is unknown, but it sets one of the most significant challenges of modern psychiatry- how to treat depression effectively, or better said, how to reduce the number of patients unresponsive to standard treatment with SSRIs or SNRIs. Over a few years, scientists investigated this bizarre phenomenon, and although some valid theories explain the resistance to treatment, there is still a huge gap in understanding the proper mechanism behind this unresponsiveness to therapy.
During the years after the rise of SSRIs, there have been a few medications that seemed promising in treating depression. One of those medications is an anesthetic discovered about 20 years before the first SSRI, fluoxetine.
Ketamine is a medication primarily used for the induction and maintenance of anesthesia. Ketamine was first synthesized in 1962 by Calvin L. Stevens, a professor of Chemistry at Wayne State University, and following FDA approval in 1970, ketamine anesthesia was extensively used for surgical procedures on American soldiers during the Vietnam War.
Even today, ketamine remains a drug of choice for some surgical procedures due to its lower respiratory depression effects compared to other anesthetics. 30 years later, its first antidepressant action was observed, and some would argue that this discovery is the single most important advance in the treatment of depression in over 50 years. Ketamine induces a so-called “dissociative anesthesia,” a state of consciousness characterized by a sense of detachment from one's physical body and the external world, also known as depersonalization and derealization.
While ketamine in moderate doses causes anesthesia, it can also significantly reduce pain in lower or sub-anesthetic doses. On the other hand, at sufficiently high doses, users may experience what is called the "K-hole", a state of dissociation with visual and auditory hallucinations similar to the effects of LSD.
What is the mechanism of action of ketamine?
Ketamine has a variety of actions in the body and the brain. To completely understand the effects of ketamine, we have to talk about one of the most abundant neurotransmitters, called glutamate.
Glutamate is the single most important excitatory neurotransmitter in our nervous system, excitatory meaning that binding to its receptor induces an excitatory reaction in our neurons. Glutamate has an important role in neuroplasticity and is involved in processes like learning and memory, but is also involved in synaptogenesis (creation of synapses) during brain development.
Glutamate acts by binding to its receptors, which are divided into three types: AMPA, NMDA, and metabotropic glutamate receptors.
While AMPA and metabotropic glutamate receptors are important for many of the glutamate functions, we will focus on their effect on NMDA receptors.
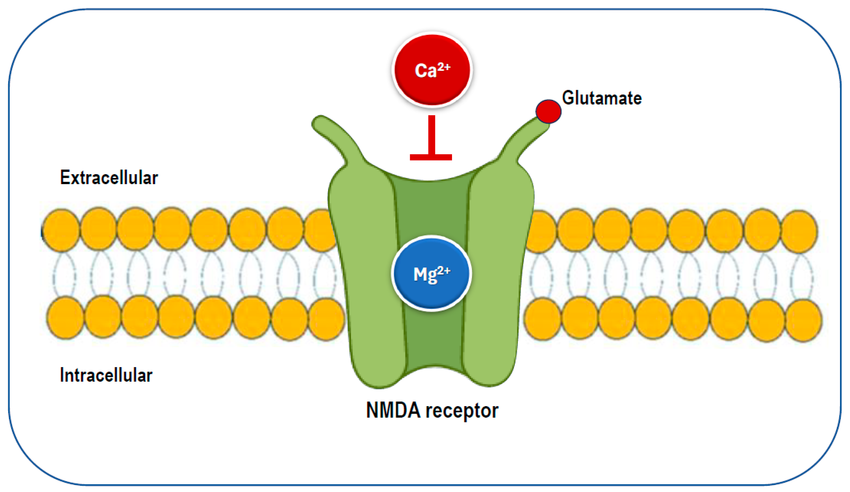
NMDA (n-methyl-d-aspartate) is an ionotropic receptor, a receptor that is built like a tunnel and opens when activated by glutamate. This opening allows many ions, like sodium or calcium ions, to pass from the extracellular space into the cytoplasm of the neuron, where they facilitate different mechanisms that change the electrical activity of the neuron.
It may sound complicated, but it is necessary to understand how ketamine works in our brains.
Ketamine is a potent anesthetic since it acts as an NMDA antagonist, preventing the activation of NMDA receptors and inhibiting the excitatory effects of glutamate we mentioned earlier.
But the true question is, how can ketamine be used to treat depression?
Apart from its antagonizing effects on NMDA glutamate receptors, ketamine acts as a so-called “dirty” or “promiscuous” drug on the brain. The term “dirty drug” is an informal name for a drug that binds to many different receptors and has a wide variety of effects and mechanisms.
One explanation for ketamine’s antidepressant effect is its mechanism of increasing the glutamate in the synapses, thus allowing it to bind to different receptors like AMPA we mentioned earlier. This mechanism allows other neurons to release a cascade of different molecules that provide better communication between neurons.
Another even more valuable effect of ketamine is its property to induce synaptogenesis and neurogenesis through molecules called neurotrophins. These molecules support the growth, survival, and differentiation of neurons but are also responsible for neuroplasticity and the formation of new memories.
Another important antidepressant effect of ketamine is a psychological one.
Patients treated with ketamine infusions usually report a warm, fuzzy-like feeling. Like being wrapped in a warm blanket and secure from all threats and anxieties in their life. Some users report a feeling that nothing is that important in life, leading some of them to new revelations about their life and their anxieties, and problems.
While the depersonalization they experience might provide a step back from reality and an objective view of their lives, this warm, soft feeling is a perfect environment for proper psychotherapy.
And the clinical findings confirm this, as we can see that psychotherapy in combination with ketamine infusions gives better results than ketamine infusions alone.
Another antidepressant property of ketamine that is worth mentioning is its hallucinogenic effect, which patients usually describe as feelings of the greater good or finding meaning in life. These psychological effects must be taken into account when talking about ketamine’s antidepressant effects, since these phenomena can break the cycle of anxiety and depression these patients struggle with.
But the most shocking aspect of ketamine treatment for refractory depression is the time it takes to see its full effect.
Unlike many standard antidepressants (like SSRIs and SNRIs) that usually take 6-8 weeks of treatment to see the effects, ketamine provides relief after the first infusion.
While ketamine provides promising results in treating depression unresponsive to standard treatment, there are some side effects you should be aware of.
Most side effects appear during the initial infusion and include high blood pressure, gastrointestinal disturbances such as nausea and vomiting, and perceptual disturbances such as feelings of time and space distortion. It is crucial to understand that ketamine has addictive properties and should be avoided in some patients with a history of substance abuse since it can lead to a counter effect.
Ketamine infusions are proven to be helpful in some patients with major depressive disorder, bipolar disorder, and some anxiety disorders, and also reduce suicidality. Nevertheless, there is still much to investigate behind ketamine’s mechanism of action, potential side effects, and other effects on the brain.
TL;DR:
About one-third of people with depression don’t respond to standard antidepressants (SSRIs/SNRIs), and the reason is still unclear. Ketamine, an anesthetic discovered in the 1960s, has emerged as a breakthrough for treatment-resistant depression. Unlike traditional antidepressants, ketamine can relieve symptoms within hours after a single infusion.
Ketamine works mainly by blocking NMDA glutamate receptors, indirectly boosting glutamate signaling through other receptors (like AMPA), which improves neural communication, promotes synaptogenesis, and enhances neuroplasticity via neurotrophins. It also has powerful psychological effects, including dissociation, feelings of warmth, safety, and meaning, which can help break cycles of depression and enhance psychotherapy outcomes.
Despite its promise, ketamine has side effects (e.g., increased blood pressure, nausea, perceptual disturbances) and addictive potential, making careful patient selection essential. While effective for some forms of treatment-resistant depression, anxiety, bipolar disorder, and suicidality, its full mechanisms and long-term effects still require further research.